Diagnosis
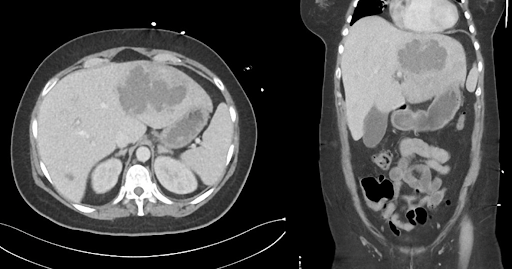
Amoebic liver abscess caused by Entamoeba histolytica, presumably acquired during NGO work in Bangladesh.
Differential diagnosis
A bacterial liver abscess is an obvious differential diagnosis, but several findings argue against this diagnosis: The patient had no known biliary infection, no intra-abdominal focus such as appendicitis or diverticulitis, and no recent sepsis. In addition, the travel history with a stay in an endemic area is clearly more suggestive of an amoebic origin.
Hepatocellular carcinoma (HCC) is extremely unlikely in a young woman without cirrhosis or hepatitis infection and without risk factors. The clinical picture with acute fever and pronounced inflammation laboratory findings also clearly argues against HCC.
A hydatid cyst (echinococcosis) is another important differential diagnosis for cystic liver lesions, especially in patients who have travelled abroad. In the present case, however, the lesion is not cystic with a multiseptate structure, but necrotic and solid-inflammatory. In addition, specific serologies and the typical calcified capsule that would indicate an echinococcal cyst are absent.
Overall, the combination of epidemiological history, clinical presentation, imaging and positive serology makes the diagnosis of amoebic liver abscess the most likely.
Treatment and clinical progression
Therapy:
- Antiparasitic treatment: Initiation of therapy with metronidazole (750 mg three times daily for 10 days).
- Concomitant antibiotics: Ceftriaxone was administered empirically for five days to treat a possible bacterial superinfection.
- Interventional therapy: As the abscess had reached a critical size, ultrasound-guided aspiration was performed to relieve pressure.
- Nutrition: Ensuring adequate hydration and calorie intake.
Progression:
After just 48 hours on metronidazole, there was a significant clinical improvement with a reduction in fever and pain symptoms. After one week, the patient's general condition was stable and the inflammation values began to normalise. After 10 days, the patient was discharged with oral maintenance therapy with paromomycin to eliminate intraluminal amoebae. Regular follow-up appointments were scheduled with her general practitioner to ensure complete regression of the abscess.